Sunday, 28 December 2008
Google Chrome 1.0.156.0 (7477)
The current release of the browser Google Chrome had problems to display the dynamically created images in the analysis section of Glucosurfer. Now the development team of Google Chrome has finally fixed these problems. The new build will be released soon. I tested the beta 1.0.156.0 (build 7477) and it was working fine.
Monday, 20 October 2008
Carbohydrate measurement in other units
The carbohydrate units (CU) or bread units (BU) are just units. You can interpret these units as any number of carbohydrates. This means it is fine to choose CU as scale even if 1CU are 15g of carbohydrates for you. Just enter the right carbohydrate factors (insulin factors) in your settings according to one of your units.
This also means that we can not tell how many carbohydrates in weight units are actually consumed by you. But you will know that one CU means a certain amount of carbohydrates.
This also means that we can not tell how many carbohydrates in weight units are actually consumed by you. But you will know that one CU means a certain amount of carbohydrates.
Wednesday, 8 October 2008
Carbohydrate measurement in USA
In the USA diabetics will log their carbohydrates in gram or another weight unit. It is not common unlike in Germany to log the carbohydrates in bread units or carbohydrate units. Therefore we decided to adapt Glucosurfer.org to support this approach.
Now you can choose to log your carbohydrates in gram or other weight units. Simply enter your amount of carbs in your weight unit. This number is multiplied with the carbohydrate factor which is calculated according to one weight unit. This means that the carbohydrate factor will be very small like 1/18 = 0.0555 but most diabetics in USA are used to this scheme.
Another difference of measuring in weight units is that you have to redefine the carbohydrate effect. In Germany one carbohydrate unit (10g=1CU) will normally increase the blood glucose by 30 mg/dL. This value has to be divided by 10 to get the increase of blood glucose per gram. For other weight units this has to be calculated accordingly.
With weight units the Glucosurfer will just ask for 'Carbs' as an abbrevation for carbohydrates that are measured in weight units.
Now you can choose to log your carbohydrates in gram or other weight units. Simply enter your amount of carbs in your weight unit. This number is multiplied with the carbohydrate factor which is calculated according to one weight unit. This means that the carbohydrate factor will be very small like 1/18 = 0.0555 but most diabetics in USA are used to this scheme.
Another difference of measuring in weight units is that you have to redefine the carbohydrate effect. In Germany one carbohydrate unit (10g=1CU) will normally increase the blood glucose by 30 mg/dL. This value has to be divided by 10 to get the increase of blood glucose per gram. For other weight units this has to be calculated accordingly.
With weight units the Glucosurfer will just ask for 'Carbs' as an abbrevation for carbohydrates that are measured in weight units.
TuDiabetes.com
I just wanted to share with you that I am now member of the growing community of TuDiabetes.com. You will find very experienced diabetics, book authors and bloggers there.
Visit Tu Diabetes - A Community for People Touched by Diabetes
Visit Tu Diabetes - A Community for People Touched by Diabetes
Friday, 27 June 2008
Behandlungsfehler bei Typ1 Diabetikern (German)
An dieser Stelle möchte ich Behandlungsfehler beleuchten, die mir bei vielen Tagebüchern aufgefallen sind. Wenn ich in den nachfolgenden Passagen von Fehlern rede, dann blende ich natürlich die jeweilige Situation der Person aus. Generell mögen es Fehler sein, aber in gleicher Weise kann es Diabetiker geben, für die bereits kleine Verbesserungen einen großen Erfolg bedeuten. Deshalb möchte ich meine Leser darum bitten die nachfolgenden Abschnitte nicht als indirekten Vorwurf zu interpretieren. Statt dessen möchte ich Denkanstöße für die eigene Behandlung vermitteln:
Fehlende Anpassung der Basalrate
Anpassungen der Basalrate sind bei sportlicher Betätigung oder Krankheit immer erforderlich.
Wer nur bei hoher körperlicher Belastung über gute Glukosewerte verfügt (z.B. bei Kanu- oder Radtouren), der muss in Ruhephasen sein Basalinsulin erhöhen um die gleichen Ergebnisse zu erzielen. Umgekehrt gilt: Wer bereits in Ruhephasen gute Glukosewerte hat, der muss bei hoher körperlicher Aktivität eine Senkung des Basalinsulins einplanen um eine Unterzuckerung zu vermeiden.
Bei fiebrigen Erkrankungen stellt der Körper mehr Glukose aus den körpereigenen Depots bereit. Folglich muss die Basalrate erhöht werden um die zusätzliche Glukose im Blut verwerten zu können.
Bei schleichender Gewichtszunahme kommt es zu einer langsamen Erhöhung des Bedarfs an Basalinsulin. Die hinzugekommenen Körperzellen benötigen einfach mehr Insulin. Nach mehreren Monaten einer solchen Entwicklung stellt sich heraus, dass die Glukosewerte nicht mehr zufriedenstellend sind. Häufig wird dieser Zusammenhang nicht erkannt. Es wird dann versucht nur die BE-Faktoren zu erhöhen, obwohl zugleich die Basalrate erhöht werden müsste.
Falsche Basalrate
die vorherigen Punkte führen in der Konsequenz dazu, dass die Basalrate nicht mehr angemessen ist. Diese Situation kann man daran erkennen, dass viele Glukoseschwankungen auftreten. Das kurzfristige Insulin wird immer öfter als Korrekturinsulin eingesetzt um die Spitzen abzufangen. Gerade bei Patienten mit Normalinsulinen sieht man häufig, dass das Normalinsulin sich überlappt und wie ein zusätzliches Basalinsulin benutzt wird. Isst der Patient an einem Tag viele Mahlzeiten, dann funktioniert die Einstellung einigermassen. Wird auf das Essen verzichtet, dann erhöhen sich die Glukosewerte dramatisch, weil schlicht und einfach Insulin fehlt.
Besonders häufig konnte ich falsche Basalraten bei Pumpennutzern beobachten. Ich möchte fast behaupten, dass 60% der Pumpennutzer davon profitieren würden, wenn ihre Pumpenprofil besser programmiert wäre. Das ist für mich eine echte Überraschung, denn gerade Pumper haben alle Möglichkeiten ihre Pumpe schnell optimal anzupassen und schnell große Erfolge zu erzielen. Warum gerade die Pumpennutzer so sehr auf die Richtigkeit ihres Pumpenprogramms vertrauen ist mir ein Rätsel. Eigentlich müsste diese Patientengruppe jedes halbe Jahr das Pumpenprogramm in Frage stellen und zusammen mit dem Diabetologen überprüfen.
Falsches Basalinsulin
Insuline und ihre Anwendung müssen zu den körperlichen Eigenschaften des jeweiligen Menschen passen.
Ein gutes Beispiel ist das Insulin Lantus. Es ist ein modernes und äußerst wirkstabiles Basalinsulin. Für die meisten Nutzer ein großer Fortschritt. Trotzdem kann man diesen Erfolg nicht auf alle Patienten übertragen. Bei manchen Patienten beträgt die Wirkung eben nicht 24, sondern beispielsweise nur 22 Stunden. Eine solche Deckungslücke ist nicht akzeptabel, weil sie immer zu einem Anstieg des Blutzuckers führt. In einem solchen Fall könnte man mit zwei Dosen Lantus (eine morgens, eine abends) arbeiten oder auf ein anderes Insulin wie Levemir wechseln.
Auch bei Levemir handelt es sich um ein modernes Insulin, welches über eine gleichmässige und zeitstabile Wirkung verfügt. Aufgrund seiner 12 Stunden Wirkung ist es für körperlich aktive Menschen besser geeignet, weil Sport oder körperliche Arbeit durch eine Senkung des Basalinsulins kompensiert werden können.
Das jeweils richtige Basalinsulin kann man durch Ausprobieren herausfinden. Ihr Diabetologe wird Sie dabei gerne unterstützen.
Falscher Spritzabstand des Basalinsulins
Es hat sich herausgestellt, dass einige Anwender von Basalinsulin nicht die notwendigen Spritzabstände einhalten. Eine Schwankung von einer Stunde sollte dabei noch kein Problem darstellen, aber darüber hinaus sind Probleme zu erwarten. Hält man sich nicht an die 12 oder 24 Stunden Wirkzeit, so hat man in einem Bereich eine Überlappung der Basalinsuline und in anderen Bereichen eine Unterversorgung mit Basalinsulin. Das führt zu einer Senkung bzw. einem Anstieg der Glukosewerte, die man sich nur durch unsere visuelle Darstellung des Insulins im Kurvenverlauf erklären kann. Ein reiner Blick in die Eintragungen des Tagebuchs kann solche Zusammenhänge nicht entlarven. Hier ist darauf zu achten, dass die Spritzabstände besser eingehalten werden.
Falsche BE-Faktoren
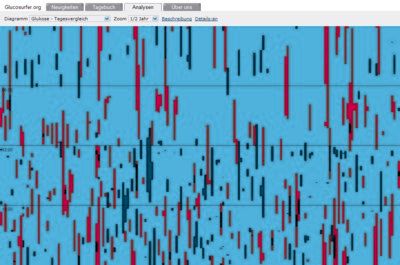
Tritt sehr häufig um 23 Uhr ein erhöhter Glukosewert auf, so sieht man im Tagesvergleich eine häufige Rotfärbung in dieser Phase des Tages. Solche Häufungen sind Hinweise auf einen falsch bemessenenen BE-Faktor um 17 bis 20 Uhr, also beim Abendbrot. Folglich kann die Erhöhung sehr einfach durch Erhöhung des BE-Faktors in diesem Zeitraum beseitigt werden. Welcher BE-Faktor genau anzupassen ist, hängt vom verwendeten Insulin ab. Ein Analoginsulin hat eine Wirkzeit von 2-3 Stunden und ein Normalinsulin wirkt 4-5 Stunden. Genau dieses Zeitfenster muss man zurückschauen um die Tagesphase zu finden in der eine Anpassung des BE-Faktors hilfreich wäre um hohe Werte zu vermeiden.
Oftmals werden BE-Faktoren für manuelle Berechnung so gewählt, dass die Kalkulation im Kopf leicht fällt. Minimale Abweichungen vom optimalen BE-Faktor führen aber zu einer qualitativ schlechteren Einstellung. Eine Abweichung um 0,2 im BE-Faktor führt bei 4 BE zu einer Spritzmenge, welche um 1 IE zu niedrig liegt. Folglich kann der Zielwert um 30 mg/dL überschritten sein. Man kann also folgende Regel aufstellen:
Beobachtung:
viel essen => 3-4 Stunden später schlechter Wert
wenig essen => 3-4 Stunden später guter Wert
Schlussfolgerung:
BE-Faktor ist im Nachkommabereich nicht ganz korrekt, denn bei hohen BE-Mengen skaliert der Fehler hoch und es kommt zu einer Unterdosierung. Folglich sollte der BE-Faktor im Nachkommabereich erhöht werden - z.b. plus 0,2
Unterschätzung der Abhängigkeiten von Glukosewerten
Ein guter Glukosewert vor dem abendlichen Schlaf führt mit größerer Wahrscheinlichkeit zu einem guten Glukosewert morgens. Möchte man also morgens gute Werte erreichen, so geht dies am einfachsten indem der abendliche Wert verbessert wird. Der vorherige Glukosewert ist quasi die Vorbedingung für die nachfolgenden Werte.
In gleicher Weise kann man feststellen, dass eine Unterzuckerung tendenziell dazu führt, dass nachfolgende Glukosewerte niedriger ausfallen. Deshalb rechnen wir bei Unterschreitung des Zielwertes auch Insulineinheiten aus dem Dosisvorschlag heraus (negative Korrektur) um den Zielwert bei der nachfolgenden Messung zu erreichen.
Kardinalfehler
Passivität ist sicherlich der größte Fehler, den ich beobachten konnte. Bei Verschlechterungen wird viel zu spät und sehr zögerlich eingegriffen. Hier wünsche ich mir eine höhere Bereitschaft zu Veränderungen. Eine Anpassung der Basalrate oder der BE-Faktoren ist schnell durchzuführen. Bei entsprechender Vorsicht lässt sich daraus sehr schnell ableiten, wie eine nachhaltige Verbesserung erreicht werden kann.
Fehlende Anpassung der Basalrate
Anpassungen der Basalrate sind bei sportlicher Betätigung oder Krankheit immer erforderlich.
Wer nur bei hoher körperlicher Belastung über gute Glukosewerte verfügt (z.B. bei Kanu- oder Radtouren), der muss in Ruhephasen sein Basalinsulin erhöhen um die gleichen Ergebnisse zu erzielen. Umgekehrt gilt: Wer bereits in Ruhephasen gute Glukosewerte hat, der muss bei hoher körperlicher Aktivität eine Senkung des Basalinsulins einplanen um eine Unterzuckerung zu vermeiden.
Bei fiebrigen Erkrankungen stellt der Körper mehr Glukose aus den körpereigenen Depots bereit. Folglich muss die Basalrate erhöht werden um die zusätzliche Glukose im Blut verwerten zu können.
Bei schleichender Gewichtszunahme kommt es zu einer langsamen Erhöhung des Bedarfs an Basalinsulin. Die hinzugekommenen Körperzellen benötigen einfach mehr Insulin. Nach mehreren Monaten einer solchen Entwicklung stellt sich heraus, dass die Glukosewerte nicht mehr zufriedenstellend sind. Häufig wird dieser Zusammenhang nicht erkannt. Es wird dann versucht nur die BE-Faktoren zu erhöhen, obwohl zugleich die Basalrate erhöht werden müsste.
Falsche Basalrate
die vorherigen Punkte führen in der Konsequenz dazu, dass die Basalrate nicht mehr angemessen ist. Diese Situation kann man daran erkennen, dass viele Glukoseschwankungen auftreten. Das kurzfristige Insulin wird immer öfter als Korrekturinsulin eingesetzt um die Spitzen abzufangen. Gerade bei Patienten mit Normalinsulinen sieht man häufig, dass das Normalinsulin sich überlappt und wie ein zusätzliches Basalinsulin benutzt wird. Isst der Patient an einem Tag viele Mahlzeiten, dann funktioniert die Einstellung einigermassen. Wird auf das Essen verzichtet, dann erhöhen sich die Glukosewerte dramatisch, weil schlicht und einfach Insulin fehlt.
Besonders häufig konnte ich falsche Basalraten bei Pumpennutzern beobachten. Ich möchte fast behaupten, dass 60% der Pumpennutzer davon profitieren würden, wenn ihre Pumpenprofil besser programmiert wäre. Das ist für mich eine echte Überraschung, denn gerade Pumper haben alle Möglichkeiten ihre Pumpe schnell optimal anzupassen und schnell große Erfolge zu erzielen. Warum gerade die Pumpennutzer so sehr auf die Richtigkeit ihres Pumpenprogramms vertrauen ist mir ein Rätsel. Eigentlich müsste diese Patientengruppe jedes halbe Jahr das Pumpenprogramm in Frage stellen und zusammen mit dem Diabetologen überprüfen.
Falsches Basalinsulin
Insuline und ihre Anwendung müssen zu den körperlichen Eigenschaften des jeweiligen Menschen passen.
Ein gutes Beispiel ist das Insulin Lantus. Es ist ein modernes und äußerst wirkstabiles Basalinsulin. Für die meisten Nutzer ein großer Fortschritt. Trotzdem kann man diesen Erfolg nicht auf alle Patienten übertragen. Bei manchen Patienten beträgt die Wirkung eben nicht 24, sondern beispielsweise nur 22 Stunden. Eine solche Deckungslücke ist nicht akzeptabel, weil sie immer zu einem Anstieg des Blutzuckers führt. In einem solchen Fall könnte man mit zwei Dosen Lantus (eine morgens, eine abends) arbeiten oder auf ein anderes Insulin wie Levemir wechseln.
Auch bei Levemir handelt es sich um ein modernes Insulin, welches über eine gleichmässige und zeitstabile Wirkung verfügt. Aufgrund seiner 12 Stunden Wirkung ist es für körperlich aktive Menschen besser geeignet, weil Sport oder körperliche Arbeit durch eine Senkung des Basalinsulins kompensiert werden können.
Das jeweils richtige Basalinsulin kann man durch Ausprobieren herausfinden. Ihr Diabetologe wird Sie dabei gerne unterstützen.
Falscher Spritzabstand des Basalinsulins
Es hat sich herausgestellt, dass einige Anwender von Basalinsulin nicht die notwendigen Spritzabstände einhalten. Eine Schwankung von einer Stunde sollte dabei noch kein Problem darstellen, aber darüber hinaus sind Probleme zu erwarten. Hält man sich nicht an die 12 oder 24 Stunden Wirkzeit, so hat man in einem Bereich eine Überlappung der Basalinsuline und in anderen Bereichen eine Unterversorgung mit Basalinsulin. Das führt zu einer Senkung bzw. einem Anstieg der Glukosewerte, die man sich nur durch unsere visuelle Darstellung des Insulins im Kurvenverlauf erklären kann. Ein reiner Blick in die Eintragungen des Tagebuchs kann solche Zusammenhänge nicht entlarven. Hier ist darauf zu achten, dass die Spritzabstände besser eingehalten werden.
Falsche BE-Faktoren
Tritt sehr häufig um 23 Uhr ein erhöhter Glukosewert auf, so sieht man im Tagesvergleich eine häufige Rotfärbung in dieser Phase des Tages. Solche Häufungen sind Hinweise auf einen falsch bemessenenen BE-Faktor um 17 bis 20 Uhr, also beim Abendbrot. Folglich kann die Erhöhung sehr einfach durch Erhöhung des BE-Faktors in diesem Zeitraum beseitigt werden. Welcher BE-Faktor genau anzupassen ist, hängt vom verwendeten Insulin ab. Ein Analoginsulin hat eine Wirkzeit von 2-3 Stunden und ein Normalinsulin wirkt 4-5 Stunden. Genau dieses Zeitfenster muss man zurückschauen um die Tagesphase zu finden in der eine Anpassung des BE-Faktors hilfreich wäre um hohe Werte zu vermeiden.
Oftmals werden BE-Faktoren für manuelle Berechnung so gewählt, dass die Kalkulation im Kopf leicht fällt. Minimale Abweichungen vom optimalen BE-Faktor führen aber zu einer qualitativ schlechteren Einstellung. Eine Abweichung um 0,2 im BE-Faktor führt bei 4 BE zu einer Spritzmenge, welche um 1 IE zu niedrig liegt. Folglich kann der Zielwert um 30 mg/dL überschritten sein. Man kann also folgende Regel aufstellen:
Beobachtung:
viel essen => 3-4 Stunden später schlechter Wert
wenig essen => 3-4 Stunden später guter Wert
Schlussfolgerung:
BE-Faktor ist im Nachkommabereich nicht ganz korrekt, denn bei hohen BE-Mengen skaliert der Fehler hoch und es kommt zu einer Unterdosierung. Folglich sollte der BE-Faktor im Nachkommabereich erhöht werden - z.b. plus 0,2
Unterschätzung der Abhängigkeiten von Glukosewerten
Ein guter Glukosewert vor dem abendlichen Schlaf führt mit größerer Wahrscheinlichkeit zu einem guten Glukosewert morgens. Möchte man also morgens gute Werte erreichen, so geht dies am einfachsten indem der abendliche Wert verbessert wird. Der vorherige Glukosewert ist quasi die Vorbedingung für die nachfolgenden Werte.
In gleicher Weise kann man feststellen, dass eine Unterzuckerung tendenziell dazu führt, dass nachfolgende Glukosewerte niedriger ausfallen. Deshalb rechnen wir bei Unterschreitung des Zielwertes auch Insulineinheiten aus dem Dosisvorschlag heraus (negative Korrektur) um den Zielwert bei der nachfolgenden Messung zu erreichen.
Kardinalfehler
Passivität ist sicherlich der größte Fehler, den ich beobachten konnte. Bei Verschlechterungen wird viel zu spät und sehr zögerlich eingegriffen. Hier wünsche ich mir eine höhere Bereitschaft zu Veränderungen. Eine Anpassung der Basalrate oder der BE-Faktoren ist schnell durchzuführen. Bei entsprechender Vorsicht lässt sich daraus sehr schnell ableiten, wie eine nachhaltige Verbesserung erreicht werden kann.
Monday, 2 June 2008
Firefox 3 - Guiness record
The browser Firefox 3 will soon be available. I really appreciate the work of the mozilla community on this new version. The browsing experience is faster due to improvements in the routines for memory management. Therefore I would like to recommend this browser to our users.
With your help Firefox 3 will set a new Guiness record for most downloads on one day.
Update:
The official date for the launch of Firefox 3 is June 17, 2008.
Saturday, 3 May 2008
Calibration of glucose devices
The calibration of metering devices for blood glucose has small side effects that I would like to describe here. Blood can be analysed in its pure or filtered form. This has effects on the blood glucose that can be measured within the blood:
I. whole blood: results from picking into the finger or other parts of the body. It contains different cells and liquid where the glucose is soluted.
II. blood plasma: results from a filtering method where cells and liquid are separated. The liquid is the plasma part that is of interest for analysis with laboratory equipment. The higher concentration of the liquid results in a higher concentration of glucose per mmol/L. Thus the blood glucose measured in plasma will be 15% higher. The reason for this approach is to eleminate the influence of the blood cell concentration. Some people have a higher concentration of blood cells than others (reflected by the haematocrit indicator). Furthermore the concentration changes in dependance of nutrition or menstruation.
The blood glucose from the finger is always whole blood. Now the manufacturer can calibrate its glucose device in two ways:
I. whole blood: its results reflect the blood glucose concentration in the finger. Only Roche and Bayer are calibrating their devices for Germany and Austria this way. For other parts of the world their devices are plasma calibrated.
II. blood plasma: its results are comparable with laboratory equipment that is analysing blood plasma. To reach this the measured value in whole blood is multiplied with 1.15. Most devices in the world are calibrated this way.
This means in conclusion that most manufacturers or countries prefer that the devices are comparable with laboratory figures. This makes sense since the users get a positive feedback that their device is still measuring fine.
In addition the plasma calibration has a positive side effect on the glucose control. The glucose values are always exagerated by 15%. This means that insulin users with correction rules are acting earlier to reduce their glucose level. Because of the percentual nature the effect increases the higher the measured glucose level is. The next table gives a comparision of the figures:
A diabetic with a blood plasma calibrated device measures 170 mg/dL. With a target value of 120 mg/dL he will apply 2 units of insulin for correction.
The same diabetic with a whole blood calibrated device would measure 150 mg/dL at the same time. With a target value of 120 mg/dL he will apply only 1 unit of insulin for correction.
Thus the use of plasma calibrated devices can lead to tighter glucose control because the values are 15% exagerated. At least it is feasible to follow this assumption. On the other side there is a small likelyhood that some hypoglycamic episodes will not be identified as that.
I. whole blood: results from picking into the finger or other parts of the body. It contains different cells and liquid where the glucose is soluted.
II. blood plasma: results from a filtering method where cells and liquid are separated. The liquid is the plasma part that is of interest for analysis with laboratory equipment. The higher concentration of the liquid results in a higher concentration of glucose per mmol/L. Thus the blood glucose measured in plasma will be 15% higher. The reason for this approach is to eleminate the influence of the blood cell concentration. Some people have a higher concentration of blood cells than others (reflected by the haematocrit indicator). Furthermore the concentration changes in dependance of nutrition or menstruation.
The blood glucose from the finger is always whole blood. Now the manufacturer can calibrate its glucose device in two ways:
I. whole blood: its results reflect the blood glucose concentration in the finger. Only Roche and Bayer are calibrating their devices for Germany and Austria this way. For other parts of the world their devices are plasma calibrated.
II. blood plasma: its results are comparable with laboratory equipment that is analysing blood plasma. To reach this the measured value in whole blood is multiplied with 1.15. Most devices in the world are calibrated this way.
This means in conclusion that most manufacturers or countries prefer that the devices are comparable with laboratory figures. This makes sense since the users get a positive feedback that their device is still measuring fine.
In addition the plasma calibration has a positive side effect on the glucose control. The glucose values are always exagerated by 15%. This means that insulin users with correction rules are acting earlier to reduce their glucose level. Because of the percentual nature the effect increases the higher the measured glucose level is. The next table gives a comparision of the figures:
| whole blood cal. | 26 | 35 | 44 | 53 | 62 | 70 | 79 | 88 | 97 | 106 |
| blood plasma cal. | 30 | 40 | 50 | 60 | 70 | 80 | 90 | 100 | 110 | 120 |
| whole blood cal. | 115 | 123 | 132 | 141 | 150 | 159 | 167 | 176 | 185 | 194 |
| blood plasma cal. | 130 | 140 | 150 | 160 | 170 | 180 | 190 | 200 | 210 | 220 |
| whole blood cal. | 203 | 211 | 220 | 229 | 238 | 247 | 255 | 264 | 273 | 282 |
| blood plasma cal. | 230 | 240 | 250 | 260 | 270 | 280 | 290 | 300 | 310 | 320 |
| whole blood cal. | 291 | 300 | 308 | 317 | 326 | 335 | 344 | 352 | 361 | 368 |
| blood plasma cal. | 330 | 340 | 350 | 360 | 370 | 380 | 390 | 400 | 410 | 420 |
A diabetic with a blood plasma calibrated device measures 170 mg/dL. With a target value of 120 mg/dL he will apply 2 units of insulin for correction.
The same diabetic with a whole blood calibrated device would measure 150 mg/dL at the same time. With a target value of 120 mg/dL he will apply only 1 unit of insulin for correction.
Thus the use of plasma calibrated devices can lead to tighter glucose control because the values are 15% exagerated. At least it is feasible to follow this assumption. On the other side there is a small likelyhood that some hypoglycamic episodes will not be identified as that.
Tuesday, 8 April 2008
Average Daily Risk Range (ADRR)
The indicator ADRR was introduced in the scientific paper Evaluation of a New Measure of Blood Glucose Variability in Diabetes by Dr. Boris Kovatchev, Erik Otto, Daniel Cox, Dr. Linda Gonder-Frederick and William Clarke.
The ADRR measures the risk induced by high variability of blood glucose readings. It tries to weigh low and high BG values in an equal fashion. Behind this are two fundamental thoughts about variability and its risks:
1) low blood glucose values are an acute risk. Furthermore patients with many low values will try to prevent this from happening. They do this by seeking higher overall regions. Thus they will seek higher target values or reduce their insulin doses. This tendency will likely degrade their HbA1c performance.
2) high variability of blood glucose readings is risky in the long term. A number of studies found that, in addition to causing cardiovascular complications, cyclic hyperglycemia is an independent contributor to chronic cardiovascular disease and increased mortality. Therefore the knowledge about the glycemic variation is important to develop strategies to narrow down the variability.
The ADRR tries to give a quality indication for both types of risks with these ranges:
Low risk: 0 <= ADRR < 20
Moderate risk: 20 <= ADRR < 40
High risk: 40 <= ADRR
Conclusion: the ADRR is an interesting indicator for risks that are not necessarily reflected by the HbA1c. By calculating the ADRR monthly patients get immediate feedback how their strategies to prevent low values and high variability have worked out for them. These positive side effects of the ADRR convinced our team to implement the ADRR in future versions of the Glucosurfer.
Update: It came to our knowledge that the ADRR is patended by the University of Virginia (USA). Therefore we have asked its Patent Foundation to grant us the right to use the ADRR in our non-commercial project. Let's hope that our project will convince the University to share its property with us and our users.
The ADRR measures the risk induced by high variability of blood glucose readings. It tries to weigh low and high BG values in an equal fashion. Behind this are two fundamental thoughts about variability and its risks:
1) low blood glucose values are an acute risk. Furthermore patients with many low values will try to prevent this from happening. They do this by seeking higher overall regions. Thus they will seek higher target values or reduce their insulin doses. This tendency will likely degrade their HbA1c performance.
2) high variability of blood glucose readings is risky in the long term. A number of studies found that, in addition to causing cardiovascular complications, cyclic hyperglycemia is an independent contributor to chronic cardiovascular disease and increased mortality. Therefore the knowledge about the glycemic variation is important to develop strategies to narrow down the variability.
The ADRR tries to give a quality indication for both types of risks with these ranges:
Low risk: 0 <= ADRR < 20
Moderate risk: 20 <= ADRR < 40
High risk: 40 <= ADRR
Conclusion: the ADRR is an interesting indicator for risks that are not necessarily reflected by the HbA1c. By calculating the ADRR monthly patients get immediate feedback how their strategies to prevent low values and high variability have worked out for them. These positive side effects of the ADRR convinced our team to implement the ADRR in future versions of the Glucosurfer.
Update: It came to our knowledge that the ADRR is patended by the University of Virginia (USA). Therefore we have asked its Patent Foundation to grant us the right to use the ADRR in our non-commercial project. Let's hope that our project will convince the University to share its property with us and our users.
Saturday, 29 March 2008
Carbohydrate bug
One new user reported that the input field for the carbohydrates disappeared. After some investigation we found out that the misconfiguration happened last week - but only new users where affected. We where able to fix the problem within minutes.
Thursday, 20 March 2008
Deutschlandradio Kultur
The well known Deutschlandradio Kultur has send a radio broadcast about Glucosurfer.org in their rubric "Elektronische Welten". It aired on March, 19 at 16:50 o'clock. You can listen to this broadcast here.
Copyright 2008

We would like to thank Stephanie Kowalewski for the time she has invested in interviews and the well made broadcast. In addition we would like to thank Dr. Klaus-Jürgen Wiefels from the German Diabetes Clinic in Düsseldorf for sharing his thoughts about the project.
We hope that many people will spread the news...
Copyright 2008
We would like to thank Stephanie Kowalewski for the time she has invested in interviews and the well made broadcast. In addition we would like to thank Dr. Klaus-Jürgen Wiefels from the German Diabetes Clinic in Düsseldorf for sharing his thoughts about the project.
We hope that many people will spread the news...
Tuesday, 18 March 2008
Therapieerfolg durch Insulinpumpen (German)
Vorbemerkung: Die nachfolgenden Ausführungen stellen keine allgemeine Behandlungsempfehlung dar. Jeder Mensch benötigt eine andere Behandlung seines Diabetes und daher ist nur ein Diabetologe oder Ernährungsberater in der Lage Ihnen individuelle Empfehlungen für Ihre Therapie zu geben. Meine Anmerkungen sind lediglich dazu geeignet Ihnen einen Denkanstoss für Ihre persönliche Behandlung zu geben.
Die optimale Einstellung des Basalprofils einer Insulinpumpe ist eine kleine Wissenschaft. Noch viel wichtiger ist aber, dass ein einmal erreichtes Optimum im Laufe der Zeit wieder verloren gehen kann. Die Gründe dafür sind vielfältig, wobei hormonelle Prozesse und Gewichtsveränderungen zu den wichtigeren Einflussgrößen gehören. Diese natürliche Dynamik macht es erforderlich, dass auch das Basalprofil in gewissen Abständen hinterfragt werden muss. Zeichnet sich beispielsweise eine starke Tendenz zu höheren Blutzuckerwerten in den Nachmittagsstunden ab, so sollte darauf geeignet reagiert werden. Am besten sind Sie mit so einer Anpassung bei einem Diabetologen aufgehoben, der Ihren Basalbedarf durch einen mehrstufigen Basalratentest ermitteln kann. Sollte Ihr Problem sich auf den halben Tag oder mehr erstrecken, so ist ein solcher Basalratentest unumgänglich.
In sonstigen Fällen: Wenn Sie umsichtig vorgehen, können Sie solche Anpassungen auch selber vornehmen. Gerade als Pumpenpatient hat man alle Möglichkeiten zur positiven Beeinflussung des Blutzuckers, weil das Pumpenprofil für jede Stunde des Tages angepasst werden kann. Es spricht also nichts dagegen einer starken Erhöhungstendenz am Nachmittag eine Erhöhung der Basalrate in den Nachmittagsstunden entgegenzusetzen. Dabei zählen nicht die schnellen Erfolge, sondern das langsame Herantasten an den tatsächlichen Basalbedarf in kleineren Schritten. Beispielsweise kann eine Zugabe von 10% Basalinsulin zu jeder Stunde des Nachmittags vorgenommen werden. Dabei sollte versucht werden den Charakter des bisherigen Profils beizubehalten und nur eine Verstärkung zu erzielen.
15:00 Uhr +10% z.B. 1 statt 0,9
16:00 Uhr +10% z.B. 1,1 statt 1,0
17:00 Uhr +10% z.B. 1,1 statt 1,0
Durch häufigeres Testen des Blutzuckers in der Zeit der Anpassung können Sie die Auswirkungen herausfinden. Es sollte zu einer kleinen positiven Veränderung des Blutzuckers kommen.
Nach zwei Tagen können Sie den nächsten Erhöhungsschritt einplanen und wieder 10% erhöhen. Innerhalb weniger Tage sollten Sie eine bessere Basalrate ermittelt haben, wobei Sie auch die Alltagstauglichkeit prüfen sollten. Wie reagieren die Werte bei etwas höherer körperlicher Aktivität usw? Seien Sie bei den Anpassungen aber bitte vorsichtig, damit keine Unterzuckerungen eintreten.
Bitte werden Sie aktiv und nutzen Sie die Möglichkeiten Ihrer Pumpe. Denken Sie daran, dass das wichtigste Argument für die Insulinpumpe der Therapieerfolg ist. Keine Krankenkasse wird Ihnen die zur Probe getragene Pumpe verweigern, wenn Sie Erfolge vorweisen können, die Sie nur mit Hilfe der Pumpeneigenschaften erreichen konnten.
Die optimale Einstellung des Basalprofils einer Insulinpumpe ist eine kleine Wissenschaft. Noch viel wichtiger ist aber, dass ein einmal erreichtes Optimum im Laufe der Zeit wieder verloren gehen kann. Die Gründe dafür sind vielfältig, wobei hormonelle Prozesse und Gewichtsveränderungen zu den wichtigeren Einflussgrößen gehören. Diese natürliche Dynamik macht es erforderlich, dass auch das Basalprofil in gewissen Abständen hinterfragt werden muss. Zeichnet sich beispielsweise eine starke Tendenz zu höheren Blutzuckerwerten in den Nachmittagsstunden ab, so sollte darauf geeignet reagiert werden. Am besten sind Sie mit so einer Anpassung bei einem Diabetologen aufgehoben, der Ihren Basalbedarf durch einen mehrstufigen Basalratentest ermitteln kann. Sollte Ihr Problem sich auf den halben Tag oder mehr erstrecken, so ist ein solcher Basalratentest unumgänglich.
In sonstigen Fällen: Wenn Sie umsichtig vorgehen, können Sie solche Anpassungen auch selber vornehmen. Gerade als Pumpenpatient hat man alle Möglichkeiten zur positiven Beeinflussung des Blutzuckers, weil das Pumpenprofil für jede Stunde des Tages angepasst werden kann. Es spricht also nichts dagegen einer starken Erhöhungstendenz am Nachmittag eine Erhöhung der Basalrate in den Nachmittagsstunden entgegenzusetzen. Dabei zählen nicht die schnellen Erfolge, sondern das langsame Herantasten an den tatsächlichen Basalbedarf in kleineren Schritten. Beispielsweise kann eine Zugabe von 10% Basalinsulin zu jeder Stunde des Nachmittags vorgenommen werden. Dabei sollte versucht werden den Charakter des bisherigen Profils beizubehalten und nur eine Verstärkung zu erzielen.
15:00 Uhr +10% z.B. 1 statt 0,9
16:00 Uhr +10% z.B. 1,1 statt 1,0
17:00 Uhr +10% z.B. 1,1 statt 1,0
Durch häufigeres Testen des Blutzuckers in der Zeit der Anpassung können Sie die Auswirkungen herausfinden. Es sollte zu einer kleinen positiven Veränderung des Blutzuckers kommen.
Nach zwei Tagen können Sie den nächsten Erhöhungsschritt einplanen und wieder 10% erhöhen. Innerhalb weniger Tage sollten Sie eine bessere Basalrate ermittelt haben, wobei Sie auch die Alltagstauglichkeit prüfen sollten. Wie reagieren die Werte bei etwas höherer körperlicher Aktivität usw? Seien Sie bei den Anpassungen aber bitte vorsichtig, damit keine Unterzuckerungen eintreten.
Bitte werden Sie aktiv und nutzen Sie die Möglichkeiten Ihrer Pumpe. Denken Sie daran, dass das wichtigste Argument für die Insulinpumpe der Therapieerfolg ist. Keine Krankenkasse wird Ihnen die zur Probe getragene Pumpe verweigern, wenn Sie Erfolge vorweisen können, die Sie nur mit Hilfe der Pumpeneigenschaften erreichen konnten.
Thursday, 13 March 2008
Potentielle Lantus Versorgungslücke (German)
Vorbemerkung: Die nachfolgenden Ausführungen stellen keine allgemeine Behandlungsempfehlung dar. Jeder Mensch benötigt eine andere Behandlung und daher ist nur ein Diabetologe oder Ernährungsberater in der Lage Ihnen individuelle Empfehlungen für Ihre Therapie zu geben. Meine Anmerkungen sind lediglich dazu geeignet Ihnen einen Denkanstoss für Ihre persönliche Behandlung zu liefern.
Das Basalinsulin Lantus ist ein modernes und sehr effektives Langzeitinsulin. Seine Wirkungsentfaltung erfolgt sehr gleichmässig und es muss nur einmal am Tag gespritzt werden. Vor allem die Langschläfer unter den Diabetikern werden diese Eigenschaft sehr schätzen.
Leider gibt es manche Menschen, bei denen Lantus nicht die gewünschte Wirkdauer von 24 Stunden besitzt. In Folge dessen gibt es im Bereich des Spritzzeitpunkts eine Unterversorgung mit Basalinsulin.
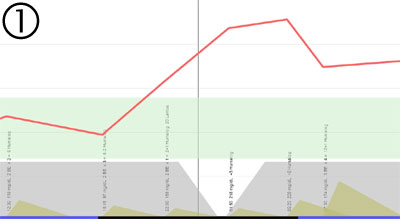
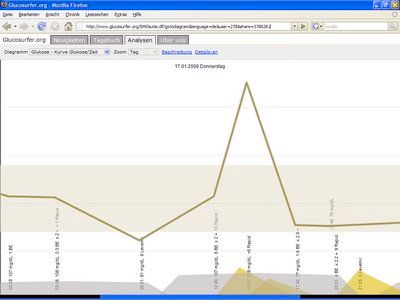
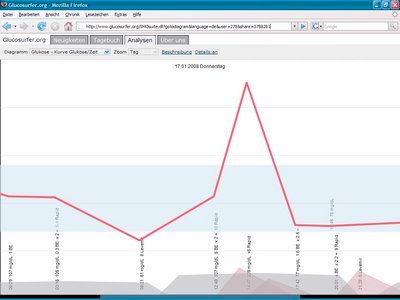
Nachfolgend ist eine solche Versorgungslücke dargestellt. Der schwarze Strich in der Mitte zeigt den Übergang zwischen zwei Tagen. Das Lantus wird vom Patienten um 22:00 Uhr gespritzt. Bis zur vollen Entfaltung seiner Wirkung vergehen mehrere Stunden. Folglich liegt die Versorgungslücke genau in der Nacht. Dies führt zu einem Anstieg des Blutzuckerspiegels von 22:00 bis 1:30 Uhr. Ab 1:30 Uhr setzt die Wirkung des um 22:00 Uhr gespritzten Lantus wieder ein. Allerdings kann das Lantus den Blutzuckerspiegel nur stabilisieren, aber nicht mehr senken. Der Patient wird also morgens mit einem hohen Wert aufwachen.
Das Problem liegt vor allem darin, dass der Patient zum Zeitpunkt der Versorgungslücke üblicherweise schläft und nicht geeignet reagieren kann. Deshalb ist es eine gute Vorgehensweise den Spritzzeitpunkt von 22:00 Uhr auf 18:00 Uhr zu verlegen. Dies kann man in mehreren Etappen vornehmen:
Tag 1: 21:00 Uhr
Tag 2: 20:00 Uhr
Tag 3: 19:00 Uhr
Tag 4: 18:00 Uhr
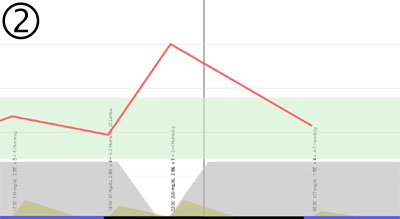
Nach der Verlegung würde sich die nachfolgende Situation ergeben. Die Versorgungslücke würde nun nach 18:00 Uhr auftreten. Dadurch hat der Patient um 22:00 Uhr noch die Möglichkeit die Blutzuckererhöhung durch eine Korrektur mit schnellem Insulin zu kompensieren. Dadurch sollte es gelingen morgens mit einem annähernd normalen Blutzuckerwert in den Tag zu starten. Gleichzeitig erhärtet sich so der Verdacht, dass die hohen Werte morgens nur der nächtlichen Versorgungslücke geschuldet sind.
Nun kann versucht werden die abendliche Versorgungslücke durch einen höheren BE-Faktor von 18:00 bis 21:00 zu kompensieren. Die Erhöhung der BE-Faktoren könnte beispielsweise wie folgt erfolgen:
18:00 Uhr von 3 auf 5
19:00 Uhr von 3 auf 5
20:00 Uhr von 2 auf 4
21:00 Uhr von 2 auf 3.5
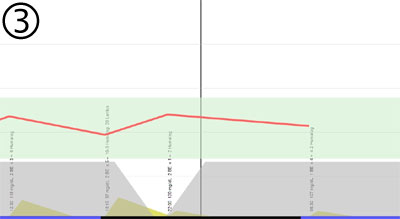
Dadurch ist mehr schnelles Insulin verfügbar, so dass um 22:00 Uhr ein normaler Blutzuckerwert erreicht werden kann - trotz der Versorgungslücke durch das Lantus. Nachfolgend ist das idealisierte Ergebnis einer Vorverlegung des Spritz-Zeitpunks und einer Erhöhung der abendlichen BE-Faktoren zu sehen:
Warnung: solche Anpassungen erfordern eine genaue Beobachtung der Blutzuckerwerte, weil die Gefahr einer Unterzuckerung besteht. In der Übergangsphase sollten die Blutzuckermessungen ab 18:00 Uhr im Abstand von 30 Minuten erfolgen!
Sollte Sie den Verdacht haben, dass eine solche Versorgungslücke bei Ihnen vorliegt, so sprechen Sie Ihren Diabetologen an, wenn Sie sich nicht trauen die obigen Punkte selber auszuprobieren. Auf jeden Fall möchte ich Sie ermutigen das Problem konstruktiv anzugehen und nach einer Lösung zu suchen.
Alternativ wäre es auch möglich die Dosis für Lantus zu halbieren und dann morgens und abends zu spritzen. Allerdings wäre dann am Wochenende kein langes Ausschlafen mehr möglich. Hier sollte man zwischen den verschiedenen Lösungansätzen abwägen und auch für diesen Lösungsansatz den Rat eines Diabetologen einholen.
Das Basalinsulin Lantus ist ein modernes und sehr effektives Langzeitinsulin. Seine Wirkungsentfaltung erfolgt sehr gleichmässig und es muss nur einmal am Tag gespritzt werden. Vor allem die Langschläfer unter den Diabetikern werden diese Eigenschaft sehr schätzen.
Leider gibt es manche Menschen, bei denen Lantus nicht die gewünschte Wirkdauer von 24 Stunden besitzt. In Folge dessen gibt es im Bereich des Spritzzeitpunkts eine Unterversorgung mit Basalinsulin.
Nachfolgend ist eine solche Versorgungslücke dargestellt. Der schwarze Strich in der Mitte zeigt den Übergang zwischen zwei Tagen. Das Lantus wird vom Patienten um 22:00 Uhr gespritzt. Bis zur vollen Entfaltung seiner Wirkung vergehen mehrere Stunden. Folglich liegt die Versorgungslücke genau in der Nacht. Dies führt zu einem Anstieg des Blutzuckerspiegels von 22:00 bis 1:30 Uhr. Ab 1:30 Uhr setzt die Wirkung des um 22:00 Uhr gespritzten Lantus wieder ein. Allerdings kann das Lantus den Blutzuckerspiegel nur stabilisieren, aber nicht mehr senken. Der Patient wird also morgens mit einem hohen Wert aufwachen.
Das Problem liegt vor allem darin, dass der Patient zum Zeitpunkt der Versorgungslücke üblicherweise schläft und nicht geeignet reagieren kann. Deshalb ist es eine gute Vorgehensweise den Spritzzeitpunkt von 22:00 Uhr auf 18:00 Uhr zu verlegen. Dies kann man in mehreren Etappen vornehmen:
Tag 1: 21:00 Uhr
Tag 2: 20:00 Uhr
Tag 3: 19:00 Uhr
Tag 4: 18:00 Uhr
Nach der Verlegung würde sich die nachfolgende Situation ergeben. Die Versorgungslücke würde nun nach 18:00 Uhr auftreten. Dadurch hat der Patient um 22:00 Uhr noch die Möglichkeit die Blutzuckererhöhung durch eine Korrektur mit schnellem Insulin zu kompensieren. Dadurch sollte es gelingen morgens mit einem annähernd normalen Blutzuckerwert in den Tag zu starten. Gleichzeitig erhärtet sich so der Verdacht, dass die hohen Werte morgens nur der nächtlichen Versorgungslücke geschuldet sind.
Nun kann versucht werden die abendliche Versorgungslücke durch einen höheren BE-Faktor von 18:00 bis 21:00 zu kompensieren. Die Erhöhung der BE-Faktoren könnte beispielsweise wie folgt erfolgen:
18:00 Uhr von 3 auf 5
19:00 Uhr von 3 auf 5
20:00 Uhr von 2 auf 4
21:00 Uhr von 2 auf 3.5
Dadurch ist mehr schnelles Insulin verfügbar, so dass um 22:00 Uhr ein normaler Blutzuckerwert erreicht werden kann - trotz der Versorgungslücke durch das Lantus. Nachfolgend ist das idealisierte Ergebnis einer Vorverlegung des Spritz-Zeitpunks und einer Erhöhung der abendlichen BE-Faktoren zu sehen:
Warnung: solche Anpassungen erfordern eine genaue Beobachtung der Blutzuckerwerte, weil die Gefahr einer Unterzuckerung besteht. In der Übergangsphase sollten die Blutzuckermessungen ab 18:00 Uhr im Abstand von 30 Minuten erfolgen!
Sollte Sie den Verdacht haben, dass eine solche Versorgungslücke bei Ihnen vorliegt, so sprechen Sie Ihren Diabetologen an, wenn Sie sich nicht trauen die obigen Punkte selber auszuprobieren. Auf jeden Fall möchte ich Sie ermutigen das Problem konstruktiv anzugehen und nach einer Lösung zu suchen.
Alternativ wäre es auch möglich die Dosis für Lantus zu halbieren und dann morgens und abends zu spritzen. Allerdings wäre dann am Wochenende kein langes Ausschlafen mehr möglich. Hier sollte man zwischen den verschiedenen Lösungansätzen abwägen und auch für diesen Lösungsansatz den Rat eines Diabetologen einholen.
Potential Lantus Gap (English)
Preliminary note: The following comments are not ment as an medical advisory. Every human needs other solutions for his health care. Therefore the diabetologist or nutritionist is the contact person for individual recommendations. My comments are meant to provoke thoughts about your treatment.
The drug called Lantus is a modern and very effective basal insulin. Its effect on the blood glucose is very steady and it needs only one injection per day. Therefore the late risers will appreciate this characteristic.
Unfortunately there are humans where the duration of the insulin effect is lower than 24 hours. This means that there is a potential gap in the supply with basal insulin. This gap happens around the typical injection time of Lantus.
The following image will show the potential impact of this gap. The black line in the middle separates two days. The Lantus will be injected around 22:00 o'clock. The insulin will need several hours to regain its effectiveness. Thus the gap is just after midnight. This causes an increase of the level of blood glucose between 22:00 and 1:30 o'clock. From 1:30 o'clock the effect of the Lantus will kick in that has been applied at 22:00 o'clock. But the Lantus can only stabilize the higher blood glucose level and it will not descrease it. The patient will experience a high blood glucose in the morning.
One problem is that the patient is sleeping when the gap is happening. Thus he can not react properly to the rise. Therefore it is recommendable to reschedule the injection of Lantus from 22:00 to 18:00 o'clock. This can be done in multiple steps:
Day 1: 21:00 o'clock
Day 2: 20:00 o'clock
Day 3: 19:00 o'clock
Day 4: 18:00 o'clock
After this shift the situation would be comparable to the next image. Now the gap happens around 18:00 o'clock. So the patient can treat the glucose increase with an injection of rapid insulin at 22:00 o'clock. This will allow him to reach a normal blood glucose in the morning. At the same time this hardens the assumption that the high glucose levels in the morning where caused by the nightly Lantus gap.
Now the patient can try to compensate the Lantus gap with an increase of the bread unit factor from 18:00 to 21:00 o'clock. This increase could be done as follows:
18:00 o'clock from 3 to 5
19:00 o'clock from 3 to 5
20:00 o'clock from 2 to 4
21:00 o'clock from 2 to 3.5
The higher level of rapid insulin should compensate the increase of glucose that is caused by the gap. In an ideal situation - like the following image - a normal glucose level can be reached at 22:00 o'clock:
Warning: this kind of changes to your treatment make it necessary to intensify your testing. To reduce the likelyhood of a hypoglycemia you should test your blood glucose level every 30 minutes from 18:00 o'clock!
Please contact your Diabetologist if you have the strong suspicion that you are experiencing this kind of Lantus gap and you are not willing to try the steps above. In any case I would like to encourage you to find a solution.
Another way to treat the gap is by applying Lantus two times a day with half of the dose. Please balance the pros and cons of these strategies and select the solution that will solve your problem in cooperation with your Diabetologist.
The drug called Lantus is a modern and very effective basal insulin. Its effect on the blood glucose is very steady and it needs only one injection per day. Therefore the late risers will appreciate this characteristic.
Unfortunately there are humans where the duration of the insulin effect is lower than 24 hours. This means that there is a potential gap in the supply with basal insulin. This gap happens around the typical injection time of Lantus.
The following image will show the potential impact of this gap. The black line in the middle separates two days. The Lantus will be injected around 22:00 o'clock. The insulin will need several hours to regain its effectiveness. Thus the gap is just after midnight. This causes an increase of the level of blood glucose between 22:00 and 1:30 o'clock. From 1:30 o'clock the effect of the Lantus will kick in that has been applied at 22:00 o'clock. But the Lantus can only stabilize the higher blood glucose level and it will not descrease it. The patient will experience a high blood glucose in the morning.
One problem is that the patient is sleeping when the gap is happening. Thus he can not react properly to the rise. Therefore it is recommendable to reschedule the injection of Lantus from 22:00 to 18:00 o'clock. This can be done in multiple steps:
Day 1: 21:00 o'clock
Day 2: 20:00 o'clock
Day 3: 19:00 o'clock
Day 4: 18:00 o'clock
After this shift the situation would be comparable to the next image. Now the gap happens around 18:00 o'clock. So the patient can treat the glucose increase with an injection of rapid insulin at 22:00 o'clock. This will allow him to reach a normal blood glucose in the morning. At the same time this hardens the assumption that the high glucose levels in the morning where caused by the nightly Lantus gap.
Now the patient can try to compensate the Lantus gap with an increase of the bread unit factor from 18:00 to 21:00 o'clock. This increase could be done as follows:
18:00 o'clock from 3 to 5
19:00 o'clock from 3 to 5
20:00 o'clock from 2 to 4
21:00 o'clock from 2 to 3.5
The higher level of rapid insulin should compensate the increase of glucose that is caused by the gap. In an ideal situation - like the following image - a normal glucose level can be reached at 22:00 o'clock:
Warning: this kind of changes to your treatment make it necessary to intensify your testing. To reduce the likelyhood of a hypoglycemia you should test your blood glucose level every 30 minutes from 18:00 o'clock!
Please contact your Diabetologist if you have the strong suspicion that you are experiencing this kind of Lantus gap and you are not willing to try the steps above. In any case I would like to encourage you to find a solution.
Another way to treat the gap is by applying Lantus two times a day with half of the dose. Please balance the pros and cons of these strategies and select the solution that will solve your problem in cooperation with your Diabetologist.
Tuesday, 11 March 2008
Activity and its influence on the insulin dose
Minor corrections have been made to the activity formula. It is planned that the percentage for every level of activity can be modified in your settings. Right now the behaviour is fixed as follows:
minor activity:
reduce the insulin dose for carbohydrates and the adjustment dose (if there is any) by 20 percent
high activity:
reduce both by 50 percent
maximum acitivity:
reduce both by 80 percent
minor activity:
reduce the insulin dose for carbohydrates and the adjustment dose (if there is any) by 20 percent
high activity:
reduce both by 50 percent
maximum acitivity:
reduce both by 80 percent
Monday, 10 March 2008
Injection To Meal Interval (Spritz-Ess-Abstand)
The Injection To Meal Interval (wait time, Spritz-Ess-Abstand = SEA) describes the time in minutes that has passed from the moment of insulin injection to the consumption of the meal.
If you use negative values for this interval this means: Meal To Injection Interval (Ess-Spritz-Abstand). Therefore it describes a situation where the carbohydrate consumption of the meal is very slow. Chocolate for example makes it in most cases necessary to inject the insulin after the meal.
The diagram Insulin Curve is simulating the insulin behaviour. The negative values will now be added to the moment of the diary entry to correctly draw the gap between intake and injection.
If you use negative values for this interval this means: Meal To Injection Interval (Ess-Spritz-Abstand). Therefore it describes a situation where the carbohydrate consumption of the meal is very slow. Chocolate for example makes it in most cases necessary to inject the insulin after the meal.
The diagram Insulin Curve is simulating the insulin behaviour. The negative values will now be added to the moment of the diary entry to correctly draw the gap between intake and injection.
Wednesday, 5 March 2008
Evolution driven by our users
Here is the roadmap of evolution that has been derived from the feedback of our users:
1. users of insulin pumps recommended that decimal doses of insulin should be supported. This innovation has already been implemented.
2. better documentation of the program used in the insulin pump: splitted insulin rate, reduced basal rate etc.
3. other diagrams to analyse the diary
4. documentation of different medicamentations.
5. support for the use of two different rapid insulins.
We are working on these steps right now. Please do not hesitate to write us your ideas to improve Glucosurfer.org
1. users of insulin pumps recommended that decimal doses of insulin should be supported. This innovation has already been implemented.
2. better documentation of the program used in the insulin pump: splitted insulin rate, reduced basal rate etc.
3. other diagrams to analyse the diary
4. documentation of different medicamentations.
5. support for the use of two different rapid insulins.
We are working on these steps right now. Please do not hesitate to write us your ideas to improve Glucosurfer.org
Friday, 15 February 2008
CSII basal profile now visible
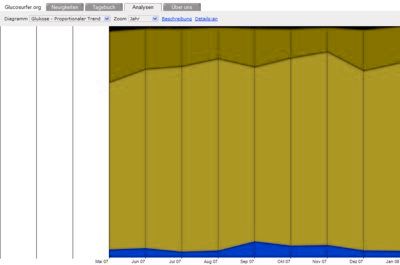
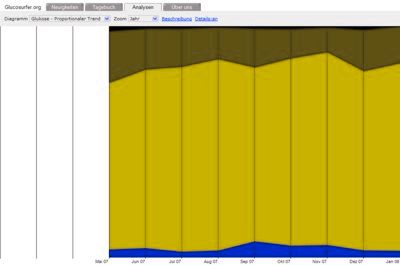
The basal profile of the Insulin pump is now visible in the diagram "Glucose - Curve Glucose/time". It is very helpfull to identify the influence of the basal program on the blood glucose.
We hope that users of Insulin pumps can identify sections in their hour profile where the basal program should be modified: increased or decreased basal rate. Step by step these small modifications can be used to optimize the blood glucose level.
We hope that users of Insulin pumps can identify sections in their hour profile where the basal program should be modified: increased or decreased basal rate. Step by step these small modifications can be used to optimize the blood glucose level.
Monday, 4 February 2008
Article in c't 4/2008
A good way to support our project is with attention in the media. The well known computer magazine c't reported about Glucosurfer.org in volume 4/2008 on page 210.
We would like to thank Urs Mansman for his supportive article that is read by a broad audience with IT background.
We would like to thank Urs Mansman for his supportive article that is read by a broad audience with IT background.
Wednesday, 30 January 2008
Color blindness: Deuteranopia (Rot-Grün-Blindheit)
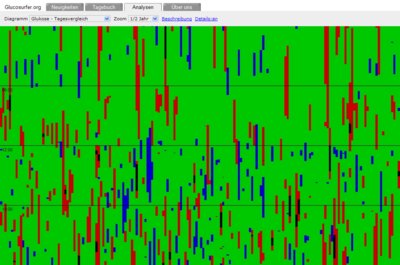
Users exhibiting Deuteranopia have a rare case of color blindness. Their perception of red/green is reduced. Which makes the distinction between these two colors difficult. We checked our diagrams with VisCheck and got good results which makes us believe that people with Deuteranopia can read our diagrams without problems:
Glucose and Insulin curve:
Comparison of days:
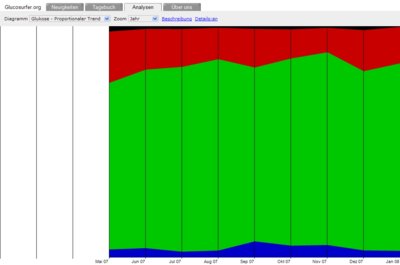
Trend:
Glucose and Insulin curve:
Comparison of days:
Trend:
Color blindness: Protanopia (Rotblindheit)
Users exhibiting Protanopia have a rare case of color blindness. Their perception of red/green is reduced. Which makes the distinction between these two colors difficult. We checked our diagrams with VisCheck and got good results which makes us believe that people with Protanopia can read our diagrams without problems:
Glucose and Insulin curve:
Comparison of days:
Trend:
Glucose and Insulin curve:
Comparison of days:
Trend:
Color blindness: Tritanopia (Blaublindheit)
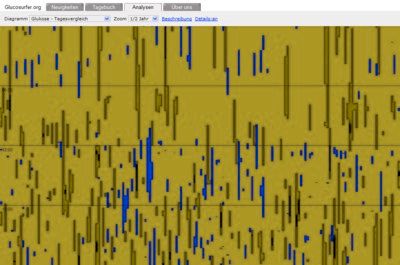
Users exhibiting Tritanopia have a very rare case of color blindness. Their perception of blue/yellow is reduced. Which makes the distinction between these two colors difficult. We checked our diagrams with VisCheck and got good results which makes us believe that people with Tritanopia can read our diagrams without problems:
Glucose and Insulin curve:
Comparison of days:
Trend:
Glucose and Insulin curve:
Comparison of days:
Trend:
Tabulator bar is now scalable
Visually impaired users often use the key combinations "Ctrl" plus "+" or "Ctrl" plus "-" to increase or decrease the font size of the page. The key combination "Ctrl" plus "0" will set the default size.
Our tabulator bar was composed of graphical elements. The problem was that these elements are not scalable. This makes them very hard to read for visually impaired users. Therefore we switched the tabulator bar to pure HTML which is fully scalable.
Our tabulator bar was composed of graphical elements. The problem was that these elements are not scalable. This makes them very hard to read for visually impaired users. Therefore we switched the tabulator bar to pure HTML which is fully scalable.
Monday, 28 January 2008
Internet Explorer: max-width of page
One user requested that we should limit the width of the page to make it more readable on wide screen displays. The CSS attribute max-width looked like the prefered way to realize this limitation - it will behave nicely on small screens. But it turned out that this attribute is not supported by the Internet Explorer. After some fruitless approaches we found this solution for our css file:
#mainContent
{
max-width:62em;
width:expression(document.body.clientWidth > 1024?"62em":"auto");
}
The max-width will work on all conforming browsers. The expression for width will only work on the Internet Explorer. The other browsers will ignore this command.
Oh dear, why is it such a problem to adopt and respect newer CSS standards?
#mainContent
{
max-width:62em;
width:expression(document.body.clientWidth > 1024?"62em":"auto");
}
The max-width will work on all conforming browsers. The expression for width will only work on the Internet Explorer. The other browsers will ignore this command.
Oh dear, why is it such a problem to adopt and respect newer CSS standards?
Friday, 25 January 2008
Insulin curves
I am very proud to announce that we have managed to display the schematical progression of the insulin curve. The diagram "Glucose - Curve" contains the insulin curve when Details:on is set. Of course these curves will not describe the reality in the blood stream of diabetics. But they are meant to provide very basic insights in the mechanisms of rapid and basal insulin. We are very sure that this visualization is helpfull for educational purposes. Furthermore very basic problems like the overlapping of insulin doses or the fade-out of basal insulin are much easier to understand.
Tuesday, 15 January 2008
Internet Explorer and YouTube videos
The security concept of the internet explorer is a mystery. The browser will give you an ActiveX warning when you embed YouTube videos into the page. The only way to solve the problem is to allow ActiveX controls on the page OR to trust the page. But this allows much more than playing the YouTube video. It will enable the page to inject every ActiveX control that it would like to inject. These controls are running directly on your computer and they have the same rights as the user that is running the internet explorer. We got around the problem by making an image of the YouTube video that is acting as a link to YouTube now. This example shows that the security concept does not enhance security. Therefore we can not recommend to use the Internet Explorer for browsing. Please use open source software like Mozilla FireFox for browsing.
Apple Safari is working
Finally we found the JavaScript problem that prevented Apple Safari users to switch between the diagrams. The diagram select box was always disabled. The problem was caused by the event handlers onmousedown and onmouseup that where set for the whole document. The problem disappeared after we have registered our handlers on the appropriate div alone. It seems unlikely that this behaviour is intended by Apple so we think that it is some sort of bug in Apple Safari.
Addon: we reported the problem and found out that our mouse handlers did not return valid return codes in all cases. Our mistake of course, but we recommend that this situation should be handled more fault tolerant by Safari.
Addon: we reported the problem and found out that our mouse handlers did not return valid return codes in all cases. Our mistake of course, but we recommend that this situation should be handled more fault tolerant by Safari.
CSII basal profile
Some users requested a basal profile for CSII treatment. Visitors of a CSII diary should be able to see this profile to look for potential problems. We have implemented the basic data structures and input fields. This means that you can already maintain your profile. In the second step these values will be visible in the diagram "Glucose - Curve Glucose/time". This will take some days to implement.
mmol/L values on mobile phones
Users with blood glucose values in mmol/L can enter these values more convenient. We split the fields in two input fields: one for the integer and one for the decimal places like we did for the BU (bread unit) values. This handling is much more convenient on mobile phones.
Subscribe to:
Posts (Atom)